Medial Ulnar Collateral Ligament Injury
(Tommy John Injury)
Anatomy
The MUCL is made up of 3 bundles. The anterior bundle is important in providing stability to the elbow in overhead throwing athletes. This bundle is most commonly injured.
Injury
Overhead athletes including baseball pitchers, javelin throwers etc. generate stress across the elbow and overtime may damage the MUCL. Injuries to the MUCL are most common at the professional or college level. This is in large part secondary to the volume of throwing as well as the velocity and stress that elite throwers place on the elbow. Initially, an athlete may feel pain in the medial aspect of the throwing arm. They may notice a drop in velocity or loss of control.

Diagnosis
A physical examination can aid in diagnosis by carefully evaluating the ligament. An MRI scan may be required to provide further information about the health of the MUCL.

Moving Valgus Stress Test
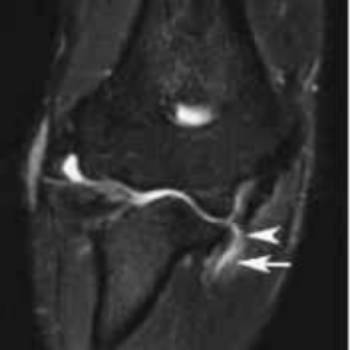
MRI showing torn MUCL
Treatment
Most injuries may be addressed through a rehabilitation program. After sufficient rest and rehabilitation the athletes complete a return to throwing program prescribed by the physician and trainers. In some situations, the elbow fails to improve with rehabilitation and reconstruction of the torn ligament is chosen. The ligament is reconstructed by harvesting the palmaris longus tendon from the wrist. The tendon is then passed through bone tunnels in and sutured in place to complete to operation.
Incision used for palmaris longs graft harvest
Illustration A and intra-operative photo B demonstrating the reconstructed MUCL ligament.
Recovery
Postoperatively the athlete is in a splint for 1 week, followed by a hinged elbow orthotic for 4 additional weeks, gradually opening the brace up to full extension during that time. The initial settings are 45 degrees to full flexion, then open 15 degrees per week until full extension is achieved. We allow full flexion immediately. Strengthening starts at week 4when the brace is discontinued. The athlete begins an interval throwing program at 16 weeks postoperatively. Usual return to pitch is about 28 weeks postoperatively.